Surgery for rotator cuff tears: repair, smooth and move, CTA arthroplasty, reverse total shoulder
Author: Frederick A. Matsen III, M.D.
The treatment of a cuff tear depends on the patient, the nature of the tear, and the symptoms being experienced.
There is an increasing amount of surgery being performed for rotator cuff tears. The rate of cuff repair surgery is increasing, even though the guidelines for performing rotator cuff surgery remain quite uncertain. The indications for rotator cuff surgery need to be tailored to the situation and needs of the individual patient. A recent review of the results of rotator cuff repair surgery may be found here.
Here are guidelines for optimizing the safety and effectiveness of surgery.
Here is a patient's perspective on planning for a rotator cuff repair and managing the aftercare.
Here is a review of the published results on the success of rotator cuff repair
There two basic surgical procedures that are considered in the management of a rotator cuff tear:
- An attempt at surgical repair of the tendon back to the area on the humerus from which it was torn
- A smooth and move procedure, also described here, in which the thickened bursa and scar tissue are removed along with the rough edges of the residual cuff and prominent humeral bone leaving a smooth convex surface to articulate with the concave coracoacromial arch coupled with a gentle manipulation of the shoulder to restore complete passive range of motion. Importantly, to preserve the stabilizing effect of the coracoacromial arch, we avoid acromioplasty or sectioning of the CA ligament.
While it has been proposed that $billions/year can be 'saved' by doing cuff repairs, we find this analysis to be flawed.
In this context, readers will be interested in this recent randomized study comparing non-operative management, acromioplasty and cuff repair in the treatment of non-traumatic cuff tears.
The strongest indication for a surgical repair is a traumatic rotator cuff tear in an otherwise healthy patient and shoulder. When a fall or other injury results in weakness or inability to use the arm normally x-rays are necessary to exclude a fracture and an MRI or ultrasound should be considered to evaluate the possibility of a rotator cuff tear. This evaluation needs to take place promptly, in that if a significant acute tear is present, the optimal time for repair is within the first six weeks before atrophy of the tendon, muscle and bone begins.
Aside from this situation, there is no urgency in considering or performing surgery for a rotator cuff tear - there is ample time for a gentle rehabilitation program and for consideration of the surgical options.
Our approach for the management of partial thickness cuff tears is shown on our blog at:
With a chronic and atraumatic cuff tears, the surgeon and the patient need to consider the likelihood that a durable repair can be achieved. Surgery may not be superior to non-operative management. We've found that some straightforward characteristics can be very informative about the quantity and quality of the tendon available for a repair attempt and have posted them on our blog at Rotator cuff tear, when to repair and when not to repair. A thorough review of the literature indicates that the quantity and quality of the residual tendon (not the surgical technique used) is the primary determinant of the durability of a surgical repair. Smoking is known to be associated with poor quality tendon and failure of repair surgery. Here is more information on the adverse effects of smoking. Older shoulders tend to have weaker cuff tendons and poorer results of repair. It is also recognized that if a repair is undertaken, the shoulder needs to be protected from loading (i.e. not used for work, play or activities of daily living) for months afterwards. From this we can see that a repair attempt should not be undertaken unless the condition of the tendon is amenable for a durable repair. It is of note that repair of larger tears requires more extreme postoperative positions to avoid excessively loading the repair. We inform patients desiring rotator cuff surgery that we will perform a repair if the quantity and quality of the tendon allows good quality cuff to be reattached to the anatomical footprint without undue tension with the arm at the side; otherwise we perform a smooth and move which allows them immediate postoperative use of the arm. This approach is supported by the many articles reviewed in this blog demonstrating that the results of attempted repair are similar whether or not the repair remains intact.
We prefer a minimally invasive open approach without acromioplasty to rotator cuff surgery in that it is expeditious, allows examination of the shoulder throughout a full range of motion, preserves the coracoacromial arch, and (because the deltoid remains intact) does not delay recovery. Our technique for cuff tendon reattachment is shown in this cuff inlay attachment image (first image below) and in greater detail in this cuff inlay attachment photo (second image below). Basically, we use an 'inlay' technique in which the tendon is securely inserted into a groove made at the normal cuff attachment site and held there securely with multiple sutures to distribute the load. More sutures = greater initial strength of the repair. Furthermore, all sutures are not equally loaded; some are more prone to tension overload.

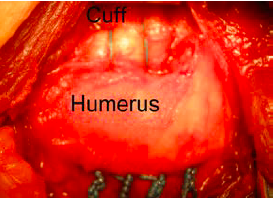
We prefer this method to 'onlay' techniques because it exposes the tendon edge to the stem cells and growth factors activated by the creation of the bony groove, because it allows for multiple sutures to create the strongest possible repair and because it allows for the possibility of some stress relaxation in the repair without loss of contact between the tendon edge and bone.
Here are some observations relevant to the need for protection of a rotator cuff repair after surgery.
An overview of the results of cuff surgery is shown here.
Smooth and move and cuff repair are also discussed at Rotator Cuff Tear: When to Repair and When to Smooth and Move the Shoulder (pdf).
There are three other procedures that are used in the management of massive rotator cuff tears:
- In the case of a massive cuff irreparable cuff tear with loss of active elevation to 90 degrees, a reverse total shoulder is considered.
- In the case of a massive cuff tear coupled with glenohumeral arthritis, a CTA arthroplasty is considered if the shoulder can be actively elevated above 90 degrees and a reverse total shoulder is considered if the shoulder is unstable or cannot be actively elevated above 90 degrees
- A latissimus dorsi tendon transfer. The role of tendon transfers for irreparable cuff tears remains unclear. Here is a presentation of the surgical method and results. And another report of the results