Repair of Rotator Cuff Tears: Surgery for shoulders with torn rotator cuff tendons can lessen shoulder pain and improve function without acromioplasty
Download this article as a pdf
In this Article:
- Overview
- Symptoms of Rotator Cuff Tears and Disease
- Diagnosis of Rotator Cuff Tears and Disease
- Treatment
- Rotator Cuff Surgery
- Physical Therapy
- Summary of Repair of Rotator Cuff Tears
- References
Overview
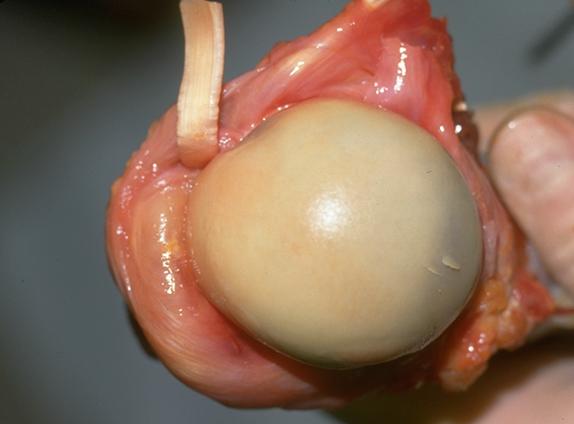
The rotator cuff is a group of four tendons that blend together to help stabilize and move the shoulder. Each of the four tendons connects a muscle originating on the shoulder blade (scapula) to part of the upper part of the arm bone (humerus). The names of these muscle-tendon components of the rotator cuff are:
- the supraspinatus which runs over the top of the ball of the shoulder joint (humeral head);
- the subscapularis which runs across the front of the humeral head; and
- the infraspinatus and the teres minor which run across the back of the humeral head.
Tears in the rotator cuff result from a combination of injury and weakening of the tendon from wear and tear, disuse, repeated use of steroid (cortisone) injection, and smoking.
The extent of injury necessary to tear the cuff depends on the quality of the tendon. Young healthy rotator cuff tendon is almost impossible to tear. However, older, multiply injured, multiply injected tendons or tendons in a smoker may tear with no injury at all. Tears in younger individuals are more likely to extend only part way through the tendon (partial thickness tears). Tears in older individuals are more likely to tear completely through the tendon (full thickness tears) and to involve multiple tendons.
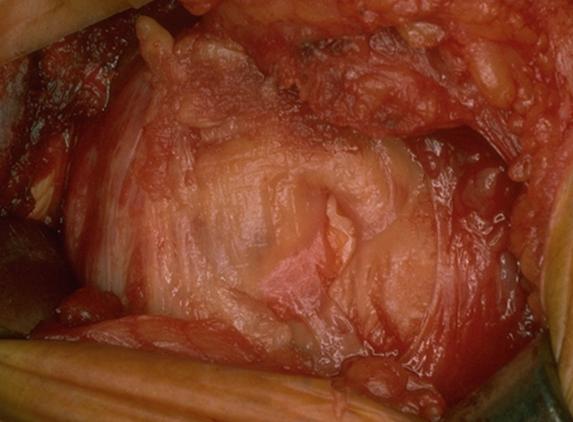
Types of Rotator Cuff Tears
Rotator cuff tears range from small to massive. Click an image below to enlarge and enter the photo gallery of rotator cuff pathology.




Full thickness tears do not heal by themselves because the muscles pull the edges of the tear apart. However it is possible for full or partial thickness tears to stabilize leaving the shoulder with reasonable comfort and function.
The more force necessary to produce a tear the more likely it is that the tear will be surgically repairable. Healthy tendon requires a major force to tear it. Tears resulting from major injury can usually be repaired successfully if surgery is not delayed more than several weeks.
Weakened degenerative cuff tissue is more easily torn even by normal activities. Durable repair of these tears may not be possible because of the lack of sufficient quantity and quality of tendon tissue. For these reasons patients should seek prompt evaluation of shoulder weakness by an experienced shoulder surgeon especially if the weakness comes on suddenly or after an injury.
A surgeon experienced in shoulder surgery can repair a rotator cuff tear if there is enough good quality tendon tissue.
- JBJS Article on Rotator Cuff Tears (PDF) (0.36 MB)
- JBJS Article on Rotator Cuff Repair (PDF) (0.18 MB)
- JBJS Article on Rotator Cuff Repair Results (PDF) (1.30 MB)
- The New England Journal of Medicine - Rotator-Cuff Failure (PDF)
- JBJS Article on Diagnosis of Impingement Syndrome of the Shoulder (PDF)
Symptoms of Rotator Cuff Tears
Rotator cuff tears are common causes of shoulder weakness and pain that can often be improved by expert shoulder surgery.
Characteristics of rotator cuff tears
Individuals with rotator cuff tears usually notice weakness pain and loss of the ability to use the shoulder for their usual activities. Commonly they have difficulty sleeping on the affected shoulder and have a limited range of active motion. Some people with rotator cuff tears notice a catching or grinding feeling when the shoulder is moved. Rotator cuff tears usually get worse over time but the rate of this progression varies widely.
Rotator cuff tears may involve the entire thickness of the tendon (full thickness rotator cuff tears) or they may be incomplete (partial thickness).
Full thickness tears may involve only part of one tendon (usually the supraspinatus). They may extend to become massive involving multiple tendons as shown in the figure.
Rotator cuff tears may be degenerative (the defect arose in tendon of poor quality) or they may be traumatic (the tear arose from a major injury to otherwise healthy tissue). Cuff tear arthropathy refers to the combination of a massive cuff tear and arthritis of the shoulder joint.
Similar conditions
Rotator cuff disease must be distinguished from shoulder arthritis, arthritis of the acromioclavicular joint, subacromial bursitis, frozen shoulder, and neck arthritis; each of which may produce similar symptoms.
- Shoulder arthritis usually causes pain and limited shoulder motion. X-rays confirm the presence of arthritis.
- Arthritis of the acromioclavicular joint usually produces pain localized to the top front of the shoulder that is made worse by using the arm in front of the body. Shoulder strength is usually normal.
- Subacromial bursitis may cause catching and pain in the shoulder but shoulder strength is maintained.
- Frozen shoulder is characterized by shoulder stiffness but the shoulder is usually strong.
- Neck arthritis with nerve impingement may cause shoulder pain and weakness that is worse when the head is held in certain positions. In this case electromyography may identify the presence of nerve involvement in the neck. Some have used the term "impingement syndrome" to refer to various types of cuff disease. However, modern diagnostic approaches usually permit a more specific diagnosis.
Incidence and risk factors
Conditions of the rotator cuff are the most common cause of problems of the shoulder. They are more likely to be found in people over the age of 40, smokers, and individuals who have had multiple steroid (cortisone) injections. People over the age of 40 who dislocate their shoulders are likely to have cuff tears. Those who have a cuff tear in one shoulder are likely to have similar problems in the opposite shoulder.
Diagnosis
A physician diagnoses rotator cuff disease by reviewing the patient's history, performing a thorough physical examination of the joint, taking the proper X-rays, and obtaining confirming imaging studies (such as a shoulder ultrasound or MRI). The examination of a shoulder with cuff disease reveals weakness or pain on exertion of the shoulder against isometric resistance. Sometimes the shoulder is stiff or noisy on movement.
X-rays of the shoulder are usually normal in the presence of cuff disease. X-rays are taken to exclude other problems. Rotator cuff tendons do not show on ordinary X-ray examinations of the shoulder.
One method for diagnosis is ultrasound. In the hands of an experienced sonographer, dynamic shoulder ultrasound is a quick safe and reliable method for documenting the status of the rotator cuff tendons. By reflecting sound waves off the tendons ,sonographic images are created as the tendons move. Defects in the tendons may be revealed on these images.
Magnetic resonance imaging (MRI) is another method for imaging the rotator cuff tendons. One risk is that some patients become claustrophobic during MRI examinations.
An additional method that has been used to evaluate the integrity of cuff tendons is shoulder arthrography. In this technique dye is injected into the joint so that leaks through the cuff can be seen on X-rays.
It is essential that the shoulder surgeon establish the diagnosis of rotator cuff disease before surgical treatment is considered.
Treatment of Rotator Cuff Tears
Medications
Medications cannot help a torn tendon heal. However, mild pain-relieving medications may make shoulders with rotator cuff tears more comfortable. Cortisone (steroid) injections in the area of the cuff tendons may lessen the discomfort from the cuff problem but may also weaken the tendon tissue. Multiple injections of steroids are discouraged for this reason.
Exercises
While prompt surgery is usually recommended for acute cuff tears in generally healthy shoulders exercises may be helpful in maintaining the flexibility and strength of joints with long-standing cuff tears. In most cases these exercises can be done in the patient's home with little equipment. Shoulder exercises are best performed gently several times a day on an ongoing basis. The exercises are not dangerous if they are performed gently so that they do not risk enlarging the cuff tear.
The figures show two examples of these exercises. The illustration on the left shows the patient using the left arm to help lift the stiff right shoulder in a forward direction. The illustration on the right shows the patient using the left arm to gently stretch the stiff right arm in external rotation using a yardstick.
Sometimes physical therapists suggest other types of therapy. Patients should learn the possible risks of these approaches as well as their costs and anticipated effectiveness.
Rotator Cuff Surgery
Possible benefits of rotator cuff surgery
When combined with a good rehabilitation effort, rotator cuff surgery allows people to regain much of the lost comfort and function in shoulders with cuff disease. In experienced hands this procedure can address the restricting scar tissue and roughness that frequently accompany cuff disease. If the quantity and quality of the tissue is good, surgery can help repair the tendon back to the bone from which it has been torn. This is most likely to succeed soon after a cuff tear in otherwise healthy shoulders of non-smokers who have not had multiple cortisone injections.
Rotator cuff surgery can improve the mechanics of the shoulder but cannot make the joint as good as it was before the cuff tear. In many cases the tendons and muscles around the shoulder have been weakened from prolonged disuse before the surgery. The tissue may be insufficient for a strong repair. In such cases the mechanics of the shoulder may be improved by carefully smoothing out the cuff area and moving the shoulder immediately after surgery so that new scars are not formed.
If the cuff is repaired it takes months before the tendon is strongly healed to the bone. During this time strengthening exercises must be avoided so that healing is not impaired. After the healing it may take months of gentle exercises before the shoulder achieves maximal improvement.
The effectiveness of the procedure depends on the health and motivation of the patient the condition of the shoulder and the expertise of the surgeon. When performed by an experienced surgeon rotator cuff surgery usually leads to improved shoulder comfort and function. The greatest improvements are in the ability of the patient to sleep, perform activities of daily living, and engage in non-contact recreational activities.
Rotator cuff surgery can optimize the comfort and function of shoulders with cuff tears.
Types of surgery recommended
When healthy tendons of the rotator cuff have been recently torn it is often possible to perform a rotator cuff repair. When a repair cannot be accomplished because of insufficient tendon quantity and quality the comfort and function of the shoulder are often improved by a "smooth and move" procedure in which the upper surface of the rotator cuff and the arm bone (humerus) are smoothed and immediate post-operative motion is used to prevent the reformation of scar tissue. Partial thickness cuff tears may be treated by detaching loose tendon fibers along with the "smooth and move" procedure.
A procedure known as acromioplasty has been advocated for the treatment of cuff disease. Recently however, the routine use of this procedure has been questioned.
Who should consider rotator cuff surgery?
Rotator cuff surgery is considered for patients with either:
- acute tears of otherwise healthy tendons or
- chronic tears that remain weak or painful after a gentle exercise program.
What happens without surgery?
Before cuff surgery is undertaken the patient needs to:
- be in optimal health
- understand and accept the risks and alternatives of surgery and
- understand the post-operative rehabilitation program.
In cases of chronic cuff tears, rotator cuff surgery can be performed whenever conditions are optimal. Sometimes the pain and stiffness from rotator cuff disease will stabilize at a level that is acceptable to the patient. In such cases the patient can delay surgery without compromising the potential for future surgery as long as the surgeon monitors the cuff tear to make sure it is not enlarging. Sequential shoulder sonography is particularly useful in sequentially following the integrity of the cuff.
In the case of an acute rotator cuff tear in otherwise healthy tissue the best chance of achieving an excellent result is surgical repair within the first month after the tear.
Rotator cuff surgery is not an emergency. If possible acute rotator cuff tears should be considered for repair within the first month after the injury. Rotator cuff surgery in chronic cuff tears is an elective procedure that can be scheduled when circumstances are optimal. In both instances the patient has time to become informed and to select an experienced surgeon.
Surgical options
Several variations of cuff surgery are used to manage cuff tendon problems. One important goal of this surgery is to allow the smooth passage of the upper arm bone (humerus) beneath what is known as the coracoacromial arch. This is usually accomplished by removing scar tissue, chronic bursitis, bony prominences, and irregular tendon edges. The combination of this smoothing with immediate, post-operative motion is known as the "smooth and move" procedure. When there is sufficient quantity and quality of tendon tissue, the torn edge of the cuff tendon is anchored to the humerus from which it was torn so that healing back to the bone can take place.
Some have advocated the repair of rotator cuff tears using shoulder arthroscopy. However, it is not clear that this more complicated approach has advantages over an expertly done direct open repair.
Others have suggested the use of various biological or artificial grafts or tendon transfers to bridge otherwise irreparable rotator cuff defects. The superiority of these complex procedures to the "smooth and move" procedure has yet to be demonstrated.
Effectiveness of Rotator Cuff Surgery
In the hands of an experienced surgeon, rotator cuff surgery can effectively restore comfort and function to the shoulder of a well-motivated patient. Often the greatest benefits are an improved ability to sleep on the affected shoulder and to perform usual activities of daily living. As long as the shoulder is cared for properly and subsequent injuries are avoided the benefit can last for decades. However, it is important to recognize that surgery cannot improve the basic quality of the tendon tissue. Thus, repair of poor-quality tissue is often followed`x` by recurrent tears.
Risks of Rotator Cuff Surgery
The risks of rotator cuff surgery include but are not limited to the following:
- infection
- injury to nerves and blood vessels
- irreparability of the rotator cuff tendon
- stiffness of the joint
- re-tear of the repaired rotator cuff
- pain
- the need for additional surgeries
There are also risks associated with anesthesia. An experienced shoulder surgery team will use special techniques to minimize these risks but cannot eliminate them completely.
Managing risk
Many of the risks of rotator cuff surgery can be managed effectively if they are promptly identified and treated.
Infections may require a "wash out" in the operating room and subsequent antibiotic treatment. Blood vessel or nerve injury may require repair. Stiffness may require exercises or additional surgery. Retear of the repaired rotator cuff may require consideration of additional surgery.
If the patient has questions or concerns about the course after surgery the surgeon should be informed as soon as possible.
How to Prepare for Rotator Cuff Surgery
Rotator cuff surgery is considered for healthy and motivated individuals in whom rotator cuff tears interferes with shoulder function.
Successful rotator cuff surgery depends on a partnership between the patient and the experienced shoulder surgeon. The patient's motivation and dedication are important elements of the partnership.
Patients should optimize their health so that they will be in the best possible condition for this procedure. Smoking should be stopped a month before surgery and not resumed for at least three months afterwards--ideally never. This is because smoking interferes with the healing of the rotator cuff repair and the strength of the cuff tendon. Any heart, lung, kidney, bladder, tooth, or gum problems should be managed before surgery. Any infection may be a reason to delay the operation.
The patient's shoulder surgeon needs to be aware of all health issues including allergies and non-prescription and prescription medications being taken. Some of these may need to be modified or stopped. For instance aspirin and anti-inflammatory medication may affect the way the blood clots.
Timing of the surgery and recovery period
Surgery for chronic cuff tears can be delayed until the time that is best for the patient's overall well-being. Acute rotator cuff tears (those that occur suddenly) have the best chance of being strongly repaired if the surgery is carried out within a month of the tear.
After rotator cuff repair the patient needs to plan on being less functional than usual for twelve or more weeks after the procedure. The shoulder should not be used with the elbow away from the side for 3 months after a rotator cuff repair. Lifting pushing pulling and many activities of daily living place stresses on the rotator cuff and can place excessive tension on the cuff repair risking failure of the repair. Driving shopping and performing usual work or chores may be difficult during this time. Plans for necessary assistance need to be made before surgery. For people who live alone or those without readily available help arrangements for home help should be made well in advance.
The shoulder surgeon should answer any questions about the surgery or the recovery period.
Costs
The surgeon's office should be able to provide a reasonable estimate of the surgeon’s fee and the hospital fee.
Surgical team
Rotator cuff surgery is a technically demanding procedure that is ideally performed by an experienced shoulder surgeon in a medical center accustomed to performing these procedures at least several times a month. Patients should inquire as to the number of rotator cuff repairs that the surgeon performs each year and the number of these procedures performed in the medical center each year.
Surgeons specializing in rotator cuff surgery may be found through university schools of medicine county medical societies state orthopedic societies or professional groups such as the American Shoulder and Elbow Surgeons.
Rotator cuff surgery is often performed in a major medical center that performs these procedures on a regular basis. These centers have surgical teams and facilities specially designed for this type of surgery. They also have nurses and therapists who are accustomed to assisting patients in their recovery from rotator cuff surgery.
Technical details of Rotator Cuff Surgery
Rotator cuff surgery is a highly technical procedure; each step plays a critical role in the outcome.
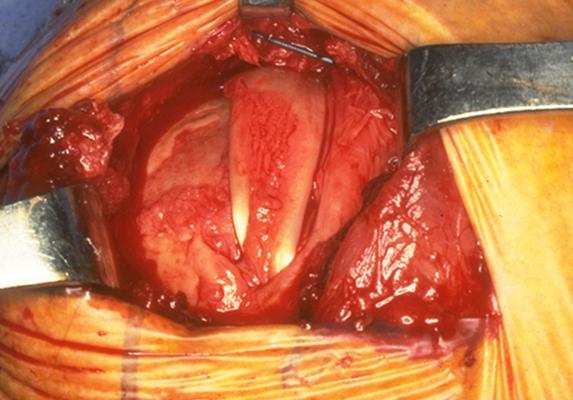
After the anesthetic has been administered and the shoulder has been prepared a cosmetic incision is made over the top front corner of the shoulder as shown in figure 13, below.
This incision allows access to the seam between the front and middle parts of the deltoid muscle. Splitting this seam allows access to the rotator cuff without detaching or damaging the important deltoid muscle which is responsible for a significant portion of the shoulder's power. All scar tissue is removed from the space beneath the deltoid and the acromion (part of the shoulder blade to which the deltoid attaches). Thickened bursa and the rough edges of the rotator cuff and humerus (upper arm bone) are also smoothed to make sure that they pass smoothly beneath the acromion and deltoid.
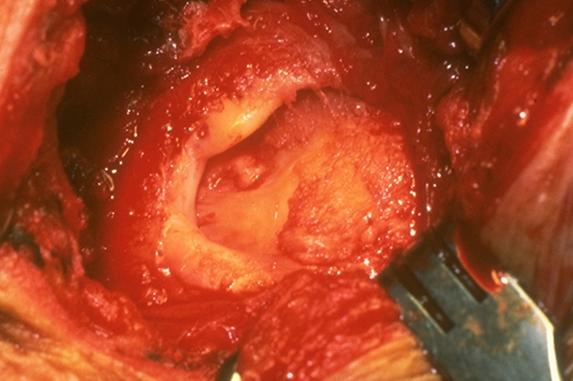
The edges of the cuff tendons are identified and the quality and quantity of the cuff tissue is determined.
The goal of the repair is to reattach good quality tendon to the location on the arm bone from which it was torn. If the tendon cannot reach this spot with the arm at the side of the body the shoulder surgeon releases the tendon from the surrounding tissues. If good quality tendon will not reach its attachment site after these releases the cuff tear is deemed to be irreparable. In this situation the useless tendon is cut out and the shoulder is again examined to assure smooth and full motion. Again achieving this smooth movement may require trimming of the tendon edges or the bone of the upper humerus. Occasionally it may be necessary to perform an acromioplasty a procedure in which part of the bone overlying the rotator cuff is removed. Acromioplasty is avoided unless it is necessary because it increases the risk of weakening the deltoid and causing scar tissue.
Click an image beow to enlarge.
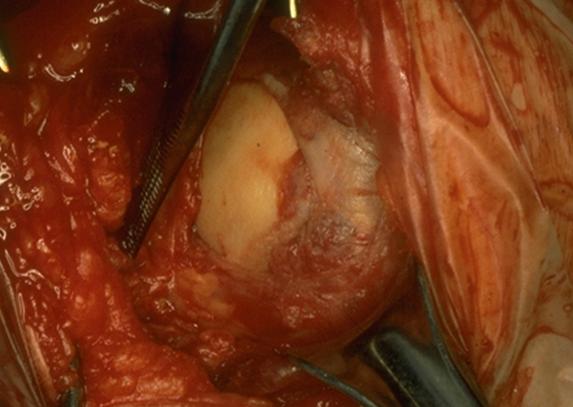
If the rotator cuff is repairable, a groove or trough is fashioned in the normal attachment site for the cuff as shown in figure 14, above.
Sutures (lengths of surgical thread) draw the edge of the tendon securely into the groove to which it is to heal. This method of attachment leaves a smooth upper edge of the cuff repair to glide beneath the acromion and deltoid and avoids possible problems with suture anchors. After the cuff is repaired the deltoid muscle and skin are closed.
Because the deltoid is not detached from the acromion in this surgical approach it is called the "deltoid on" approach.
Anesthetic
Rotator cuff surgery may be performed under a general anesthetic or a brachial plexus nerve block. A brachial plexus block can provide anesthesia for several hours after the surgery. The patient may wish to discuss their preferences with the anesthesiologist before surgery.
Length of rotator cuff surgery
Rotator cuff surgery usually takes approximately one hour. However the preoperative preparation and the postoperative recovery may add several hours to this time. Patients often spend two hours in the recovery room and about two days in the hospital after surgery. Recovery of comfort and function after cuff surgery continues for a year after surgery.
Pain Management during and after Rotator Cuff Surgery
Rotator cuff surgery is a major surgical procedure that involves cutting of skin, release of scar tissue, and suturing of tendons and bone. The pain from this surgery is managed by the anesthetic and by pain medications. Immediately after surgery strong medications (such as morphine or Demerol) are often given by injection. Within a day or so oral pain medications (such as hydrocodone or Tylenol with codeine) are usually sufficient.
Initially pain medication is administered usually intravenously or intramuscularly. Sometimes patient controlled analgesia (PCA) is used to allow the patient to administer the medication as needed. Hydrocodone or Tylenol with codeine are taken by mouth. Intravenous pain medications are usually needed only for the first day or two after the procedure. Oral pain medications are usually needed only for the first two weeks after the procedure.
Click the image below to enlarge.
Pain medications can be very powerful and effective. Their proper use lies in the balancing of their pain relieving effect and their other less desirable effects. Good pain control is an important part of the postoperative management.
Pain medications can cause drowsiness slowness of breathing difficulties in emptying the bladder and bowel nausea vomiting and allergic reactions. Patients who have taken substantial narcotic medications in the recent past may find that usual doses of pain medication are less effective. For some patients balancing the benefit and the side effects of pain medication is challenging. Patients should notify their surgeon if they have had previous difficulties with pain medication or pain control.
Hospital stay after Rotator Cuff Surgery
After surgery the patient spends an hour or so in the recovery room. A drainage tube is sometimes used to remove excess fluid from the surgical area. The drain is usually removed on the second day after surgery. Bandages cover the incision. They are usually changed the second day after surgery.
Recovery and rehabilitation in the hospital
Shoulder motion soon after rotator cuff surgery helps achieve best possible shoulder function. Shoulders with cuff disease may have substantial scarring and may be stiff. One of the major goals of rotator cuff surgery is to relieve any stiffness. However after surgery scar tissue will tend to recur and limit movement unless motion is started immediately. This early motion is facilitated by the complete surgical removal of the scar tissues so that after surgery the patient needs only to maintain the range of motion achieved at the operation.
A continuous passive motion (CPM) machine is often used to gently move the shoulder in the recovery room immediately after surgery. The CPM shown in figure 15 above and in the video clip below is continued for the first few days after surgery whenever the patient is in bed.
During the hospitalization the patient learns a simple rehabilitation program that will be used to maintain the range of motion at home after discharge.
Figure 16 below shows the exercises used to maintain elevation and rotation of the arm. On the day of surgery or on the day after the physical therapist teaches the patient gentle range of motion exercises. Usually the patient is shown how to stretch the shoulder forward and out to the side preventing stiffness and adhesions.
Continuous Passive Motion Machine Video Clip
Hospital discharge
Patients are discharged as soon as:
- the incision is dry
- the shoulder is comfortable with oral pain medications
- the patient feels comfortable with the plans for managing the shoulder
- the patient can perform the range of motion exercises and
- the home support systems for the patient are in place.
Discharge is usually on the second or third day after surgery.
Convalescent assistance
Walking and use of the arm (with the elbow at the side) for gentle activities are encouraged soon after surgery.
If a cuff repair has been performed the arm must be used only with the elbow at the side and only for very gentle activities so that the repair is protected. These precautions remain in place for three months until the initial healing of the cuff repair is complete.
The patient's specific limitations can be specified only by the surgeon who performed the procedure. It is important that the repaired tendons not be challenged until they have had a chance to heal. Usually the patient is asked to lift nothing heavier than a cup of coffee (with the elbow at the side) for the first three months after the surgery.
Management of these limitations requires advance planning to accomplish the activities of daily living during the period of recovery.
Patients usually require some assistance with self-care activities of daily living shopping and driving for approximately three months after surgery. Patients usually go home after this surgery especially if there are people at home who can provide the necessary assistance or if such help can be arranged through an agency. In the absence of home support a convalescent facility may provide a safe environment for recovery.
Recovery of comfort and function after rotator cuff surgery continues for many months after the surgery. Improvement in some activities may be evident as early as three months. With persistent effort patients make progress for as long as a year after surgery.
Effects of general health on healing
The healing after rotator cuff surgery can be compromised by smoking, poor nutrition, and medications such as cortisone. Diabetes can cause additional scar tissue. Heart and lung disease, as long as they are well managed, do not seem to have an effect.
The rehabilitation after rotator cuff surgery is carried out largely by the patient.
Physical therapy
Shoulders with rotator cuff disease may be stiff. One of the major goals of rotator cuff surgery is to relieve much of this stiffness. However after surgery scar tissue will tend to recur and limit movement unless motion is started immediately. This early motion is facilitated by the complete surgical removal of the scar tissue so that after surgery the patient needs only to maintain the range of motion achieved at the operation. Later on once the shoulder is comfortable and flexible and after the cuff repair has healed (usually three months after surgery) strengthening exercises and additional activities are started.
Rehabilitation options
It is often most effective for the patient to carry out their own exercises so that they are done frequently effectively and comfortably. Usually a physical therapist or the surgeon instructs the patient in the exercise program and advances it at a rate that is comfortable for the patient.
Can rehabilitation be done at home?
In general the exercises are best performed by the patient at home. Occasional visits to the surgeon or therapist may be useful to check the progress and to review the program.
Usual response
Patients are almost always satisfied with the increases in range of motion comfort and function that they achieve with the exercise program. If the exercises are uncomfortable difficult or painful the patient should contact the surgeon promptly.
Risks
This is a safe rehabilitation program with little risk
Duration of rehabilitation
For the first twelve weeks after surgery emphasis is placed on optimizing the flexibility and range of motion of the shoulder through gentle stretching exercises. After three months these stretching exercises are continued and strengthening exercises are added (see movies 2-5).
Once the range of motion and strength goals are achieved the exercise program can be cut back to a minimal level. However gentle stretching is recommended on an ongoing basis.
Shoulder Exercises for Rehabiliation after Rotator Cuff Repair
The video box below is a playlist of 4 shoulder exercise videos. Watch the videos below or on our youtube channel.
Returning to ordinary daily activities
In general patients are able to perform gentle activities of daily living with the operated arm at the side starting two to six weeks after surgery. Walking with the arm protected is strongly encouraged. Driving should wait until the patient can perform the necessary functions comfortably and confidently. Recovery may take three months if the surgery has been performed on the right shoulder because of the increased demands on the right shoulder for shifting gears.
With the consent of their surgeon patients can often return to activities such as swimming golf and tennis at six months after their surgery.
Long-term patient limitations
Patients should avoid activities that involve major impact (chopping wood contact sports sports with major risk of falls) or heavy loads (lifting of heavy weights heavy resistance exercises). These activities may increase the chance of repeat rotator cuff tear.
Physical Therapy Costs
The surgeon and therapist should provide information on the usual cost of the rehabilitation program. The program is quite cost-effective because it is based heavily on home exercises. Rotator cuff surgery can help restore comfort and function to shoulders with rotator cuff tears.
Summary of rotator cuff surgery for rotator cuff tears
In the hands of an experienced surgeon rotator cuff surgery can be a most effective method for restoring comfort and function to shoulders with rotator cuff tears in a healthy and motivated patient. Pre-planning and persistent rehabilitation efforts will help assure the best possible result for the patient.
References
- Churchill R. S. E. V. Fehringer et al. (2004). "Rotator cuff ultrasonography: diagnostic capabilities." J Am Acad Orthop Surg 12(1): 6-11.
- Clark J. J. A. Sidles et al. (1990). "The relationship of the glenohumeral joint capsule to the rotator cuff." Clin Orthop Relat Res(254): 29-34.
- Duckworth D. G. K. L. Smith et al. (1999). "Self-assessment questionnaires document substantial variability in the clinical expression of rotator cuff tears." J Shoulder Elbow Surg 8(4): 330-3.
- Goldberg B. A. S. B. Lippitt et al. (2001). "Improvement in comfort and function after cuff repair without acromioplasty." Clin Orthop Relat Res(390): 142-50.
- Goldberg B. A. R. J. Nowinski et al. (2001). "Outcome of nonoperative management of full-thickness rotator cuff tears." Clin Orthop Relat Res(382): 99-107.
- Harryman D. T. 2nd C. M. Hettrich et al. (2003). "A prospective multipractice investigation of patients with full-thickness rotator cuff tears: the importance of comorbidities practice and other covariables on self-assessed shoulder function and health status." J Bone Joint Surg Am 85-A(4): 690-6.
- Harryman D. T. 2nd L. A. Mack et al. (1991). "Repairs of the rotator cuff. Correlation of functional results with integrity of the cuff." J Bone Joint Surg Am 73(7): 982-9.
- Harryman D. T. 2nd F. A. Matsen 3rd et al. (1997). "Arthroscopic management of refractory shoulder stiffness." Arthroscopy 13(2): 133-47.
- Hollister M. S. L. A. Mack et al. (1995). "Association of sonographically detected subacromial/subdeltoid bursal effusion and intraarticular fluid with rotator cuff tear." AJR Am J Roentgenol 165(3): 605-8.
- Kilcoyne R. F. and F. A. Matsen 3rd (1983). "Rotator cuff tear measurement by arthropneumotomography." AJR Am J Roentgenol 140(2): 315-8.
- Largacha M. I. M. t. Parsons et al. (2006). "Deficits in shoulder function and general health associated with sixteen common shoulder diagnoses: a study of 2674 patients." J Shoulder Elbow Surg 15(1): 30-9.
- Mack L. A. M. K. Gannon et al. (1988). "Sonographic evaluation of the rotator cuff. Accuracy in patients without prior surgery." Clin Orthop Relat Res(234): 21-7.
- Mack L. A. and F. A. Matsen 3rd (1995). "Rotator cuff." Clin Diagn Ultrasound 30: 113-33.
- Mack L. A. F. A. Matsen 3rd et al. (1985). "US evaluation of the rotator cuff." Radiology 157(1): 205-9.
- Mack L. A. D. A. Nyberg et al. (1988). "Sonographic evaluation of the rotator cuff." Radiol Clin North Am 26(1): 161-77.
- Mack L. A. D. A. Nyberg et al. (1988). "Sonography of the postoperative shoulder." AJR Am J Roentgenol 150(5): 1089-93.
- McCallister W. V. I. M. Parsons et al. (2005). "Open rotator cuff repair without acromioplasty." J Bone Joint Surg Am 87(6): 1278-83.
- Norquist B. M. B. A. Goldberg et al. (2000). "Challenges in evaluating patients lost to follow-up in clinical studies of rotator cuff tears." J Bone Joint Surg Am 82(6): 838-42.
- Smith K. L. D. T. Harryman 2nd et al. (2000). "A prospective multipractice study of shoulder function and health status in patients with documented rotator cuff tears." J Shoulder Elbow Surg 9(5): 395-402.
- Viola R. W. K. C. Boatright et al. (2000). "Do shoulder patients insured by workers' compensation present with worse self-assessed function and health status?" J Shoulder Elbow Surg 9(5): 368-72.
Follow our blog
http://shoulderarthritis.blogspot.com/
On which we try to provide the best and most current information on shoulder arthritis.
See: The Rotator Cuff Tear Book at
http://shoulderarthritis.blogspot.com/2013/12/the-rotator-cuff-tear-book.html
Contact
If you have questions regarding this article, feel free to email Frederick A. Matsen III M.D. at matsen@uw.edu.